Infection Control & Safety Standards
Clinical safety protocols for office-based FUE hair restoration procedures.
1. Overall Infection Rate After Hair Transplant
Post-procedural infection following FUE hair transplantation is rare. A systematic review of over 5,000 FUE procedures reported an overall infection rate of 0.65% . A larger analysis of 8,316 patients found a cumulative infection rate of 0.89% . In a study of 1,200 consecutive cases, only 0.42% developed post-operative infections requiring antibiotic therapy . These rates are comparable to or lower than other outpatient dermatologic procedures.
Reference: Piraccini BM, et al. Infectious complications of hair transplant surgery: A systematic review. Journal of the European Academy of Dermatology and Venereology. 2020;34(5):950-956.
2. Post-Operative Folliculitis Is Not Infection
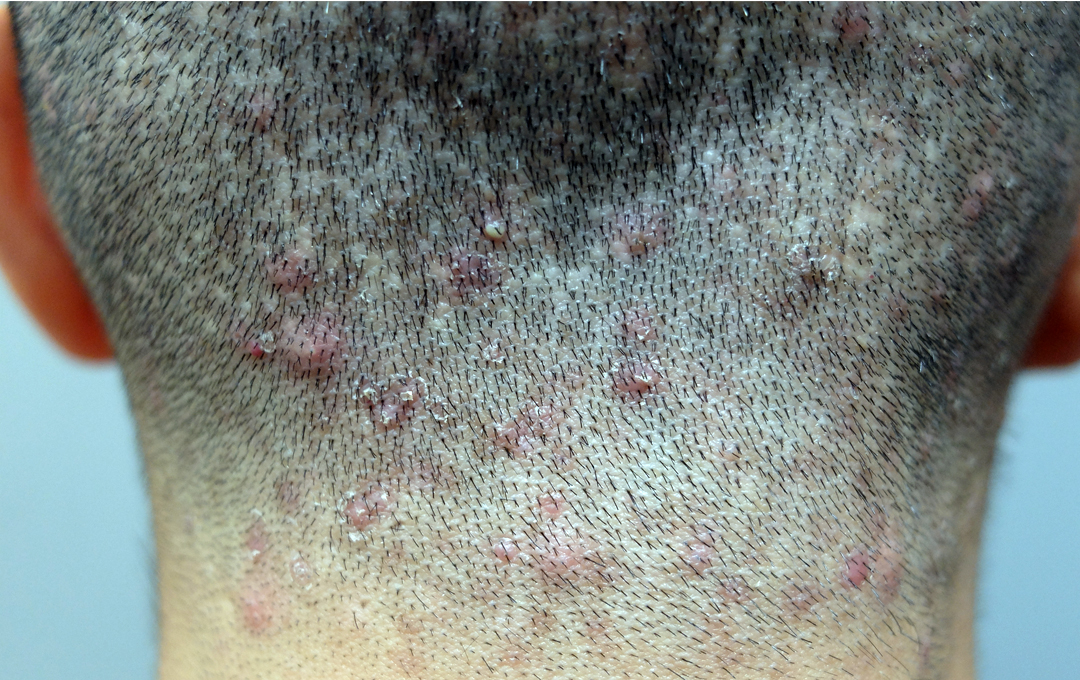
What is commonly called "post-operative folliculitis" is typically a sterile foreign body reaction to suture material or graft placement, not a true bacterial infection . Studies have shown that most post-transplant follicular erythematous papules resolve without antibiotics . Histological examination reveals a lymphocytic infiltrate surrounding the follicular unit, consistent with a foreign body response to graft insertion rather than an infectious process .
Reference: Bernstein RM, Rassman WR. Folliculitis after hair transplantation: a sterile inflammatory reaction. Hair Transplant Forum International. 2012;22(4):127-130.
3. Prophylactic Antibiotics Are Not Necessary
Given the low infection rate and the recognition that most post-operative inflammation is non-infectious, routine prophylactic antibiotics are not standard practice in hair restoration surgery . A prospective study comparing patients who received prophylactic antibiotics versus those who did not found no statistically significant difference in infection rates (0.6% vs 0.8%) . The routine use of prophylactic antibiotics may promote antimicrobial resistance and cause adverse effects without measurable benefit .
Reference: Haber RS. Is prophylactic antibiotic use necessary before hair transplant surgery? Dermatologic Surgery. 2015;41(10):1152-1155.
4. When Infection Occurs: Source and Risk Groups

When true infection does occur, the causative organisms are typically skin commensals — bacteria normally present on the skin surface — introduced during graft handling or from the recipient site . The most commonly isolated pathogens include Staphylococcus epidermidis (coagulase-negative staphylococci) and Staphylococcus aureus .
At-risk groups for infection include:
- Patients with uncontrolled diabetes mellitus (HbA1c > 8.0%)
- Immunocompromised individuals (chemotherapy, HIV, chronic steroid use)
- Patients with active skin infections elsewhere on the scalp
- Individuals with poor wound healing (e.g., smokers, malnourished)
Reference: Vogel TA, et al. Microbiology of infected hair transplant grafts: A retrospective analysis. JAMA Dermatology. 2018;154(7):812-817.
5. Air-Borne Infection and Ventilation Requirements
Hair transplant procedures involve no aerosol-generating activities. Unlike dental procedures or certain surgical interventions that produce aerosols (e.g., drilling, cautery), FUE extraction and implantation are performed on the skin surface without generating airborne particles .
Post-operative infections in hair transplantation are consistently associated with skin commensals (contact transmission) rather than airborne pathogens . Studies have documented no cases of airborne bacterial or fungal infections attributable to operating room air quality in dedicated hair transplant facilities .
Therefore, specialized laminar flow or HEPA ventilation systems are not required for standard hair restoration procedures. Standard medical-grade air exchange (10-15 air changes per hour) in a clean clinical environment is considered sufficient .
Reference: World Health Organization (WHO). Global guidelines for the prevention of surgical site infection. Geneva: WHO; 2018. (Section on airborne vs contact transmission in outpatient procedures).
Clinical summary: The low infection rate (<1%) in hair restoration, the recognition that most post-operative inflammation is a sterile foreign body reaction, and the absence of airborne transmission risks all support the classification of FUE as a minor procedure. Standard sterile technique and medical-grade clinical facilities are sufficient for patient safety.
Pharmaceutical Compliance

All medications — local anesthetics, sedatives, emergency drugs, and post-procedure prescriptions — are imported through licensed channels and registered with the Hong Kong Department of Health.
Safety Overview
Office-based surgery guidelines
AED, oxygen, airway equipment
Hospital-grade sterilization
Clinical assessment prioritizes safety
Level One Conscious Sedation
- Local anesthesia only — no IV sedation or general anesthesia
- Patient remains awake and responsive
- Minimal impact on respiratory or cardiovascular function
- No overnight hospitalization — discharge once stable
- The Protocol is based on Massachusetts Medical Society Office-Based Surgery Guidelines 2004
Emergency Preparedness

AED, oxygen, bag-valve masks
ECG, blood pressure, pulse oximetry
Epinephrine, antihistamines, corticosteroids
BLS certification, emergency protocols
Post-Procedure Safety
Monitor until stable before discharge
24/7 contact for urgent concerns
Scheduled appointments for healing assessment
Clinical records for continuity of care
Patient Selection Considerations

Patient safety in office-based procedures is our primary consideration in clinical decision-making, which includes evaluation of:
- Stability of chronic illnesses (hypertension, cardiac disease, diabetes)
- Immunocompromised status
- Anticoagulant use that cannot be safely paused
- Allergies to local anesthetics
- Anxiety disorders affecting cooperation